

Beyond Global Public Goods
Beyond Global Public Goods
Part 2: A Country Cost Curve for International Spending

Hassan Damluji & Jonathan Glennie
In our last essay, we set out the case for ending the dichotomy between Global Public Goods and Development Assistance, arguing instead for a “Scale of Global Common Benefit” that can apply to all international public spending. But what does that mean for particular countries considering where to invest scarce resources? And how does it help build the case for “beyond aid” financing for global priorities? For that we need a Country Cost Curve, which is the subject of this follow-up essay.
At the height of the COVID-19 pandemic, one of us (Hassan) was tasked with building support from high income countries to contribute to COVAX, a global scheme to provide COVID-19 vaccines rapidly and free of charge to poorer countries. The dominant advocacy line, parroted by bigwigs and journalists, was that rich countries should “spend billions to save trillions”. Ending the pandemic everywhere was a Global Public Good, we were told, meaning it was in everyone’s interest, if they could afford it, to fund vaccines for the rest.
In reality, though, COVAX was woefully underfunded. All available vaccine manufacturing capacity was being captured either by countries who could afford to buy it (mostly in Europe and North America) or those who could prevent it from being shared (India, the world’s largest vaccine manufacturer, simply banned exports). The catchy line that “no one is safe until everyone is safe” worked well in TV interviews, but the dollar reality showed that Europe & North America were unconvinced that they would suffer if Africans, Latins and Asians remained unvaccinated. Rich countries had reverted to their default way of thinking: helping poor countries was a matter of “foreign aid”, and not a national priority.
The most frustrating thing, watching this unfold, was that no one seemed to be interested in doing the maths, to improve on the lazy “spend billions to save trillions”. We knew what the cost of equitable access was – about $32 billion including vaccines, tests and treatments. But the benefits were just meant to be obvious: “trillions”, “everyone safe” a “global public good”. It wasn’t good enough.
To fill this gap, Hassan commissioned the Eurasia Group to come up with a properly researched estimate for the dollar benefits of vaccinating people in poorer countries to ten major contributors. This, for the first time, made a credible case for countries spending on COVAX, not as foreign aid, but as a national priority. The benefits to rich countries were not in the trillions, but they were still huge: just these ten countries stood to gain 12 times what they spent (even if they covered all of the costs between them).
This lone study was not enough to get COVAX fully funded. But it has helped us at Global Nation to conceptualize a new approach to advocacy which we believe can, over time, build the case for the kinds of international spending the world needs to tackle global challenges.
If we are to break free of the limits of “foreign aid” and make international expenditure a matter of national priority for governments, we need to make a much better case for the return on investment to the paying country.
That is why we are calling for development economists and advocates to get behind a new approach to international spending on global objectives, which we call the “Country Cost Curve for International Spending”.
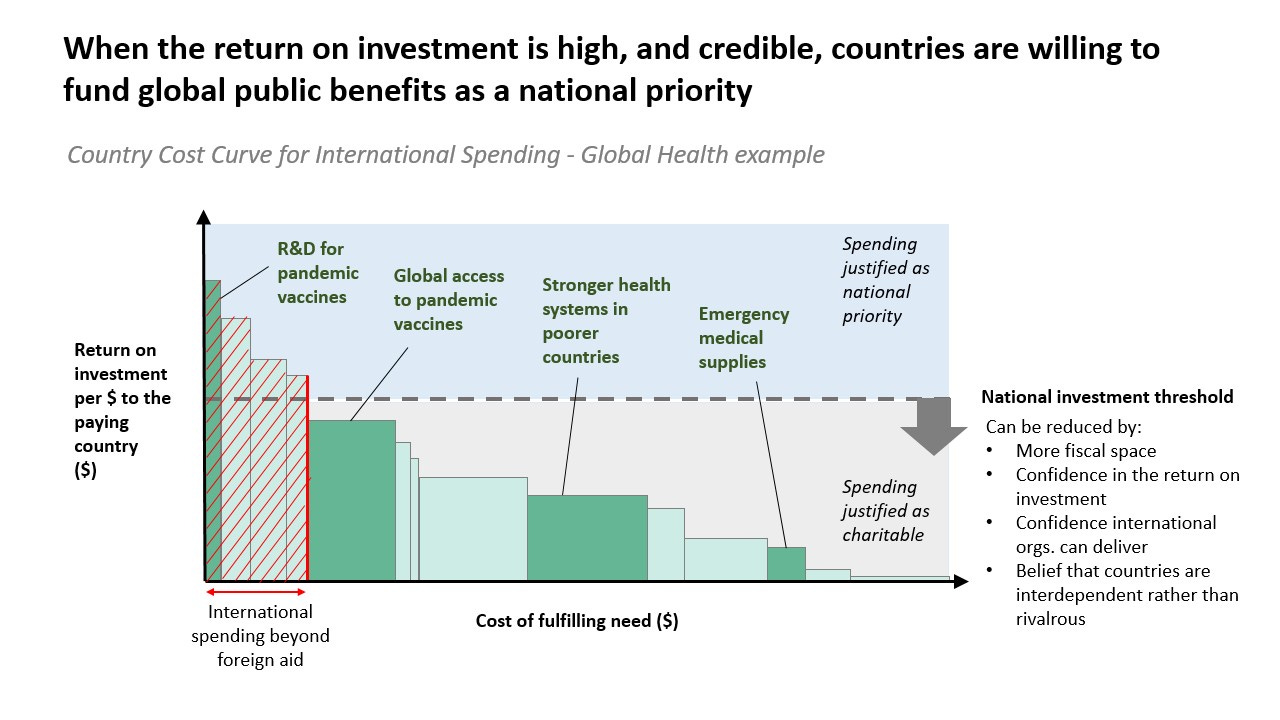
The chart below shows schematically how it works. Every international spending priority is evaluated in terms of how much it would cost to deliver (COVAX, for example, was asking for $32 billion dollars to vaccinate the populations of relatively poor countries), and what the benefits would be to paying countries (according to the Eurasia Group study, the US, for example, stood to gain a little over $200 billion over 5 years for its share of the $32 billion overall spend). The different spending priorities can then be arranged as boxes in the chart below. The total cost is the width of the box (the x-axis) and the benefit to the paying country per dollar spent is the height of the box (the y-axis). The area of the box is the total benefit to the paying country.
It is of course true that benefits will come in many shapes and sizes and not all will be economic. Lives lost, livelihoods ruins by floods or disease: there is something uncomfortable about lumping all of these into a dollar denominated “return on investment”. And yet it is also hugely clarifying as an aid when making spending decisions to be able to prioritize different options by how much impact they have. Nuance is important, but when deciding between options, comparability is key. So this approach requires putting a dollar figure to the various types of impact of different spending needs, while acknowledging that this is an imperfect way of valuing all things.
Given that these are international spending priorities on the Scale of Global Common Benefit, there will of course be significant returns accruing to countries other than the paying country. But here we are focused on the returns to the payer, which we could call the “self-interest case” for contributing.
The self-interest case is high for priorities on the left of the graph, like funding R&D for pandemic vaccines. In fact, for this example, the self-interest was so obvious that countries didn’t pause to analyze the financials. Even protectionist governments like Donald Trump’s just got on with pumping money into developing new vaccines – too many, it later turned out, as many of the vaccines were effective, and the constraint was manufacturing capacity, not different vaccines to choose from.
On the right hand side of the chart, the self-interest case is lower. Sending emergency medical supplies to a far-off island affected by a hurricane, for instance, may not bring much benefit directly to a foreign contributor. That doesn’t mean the foreign contributor shouldn’t contribute; it just means it will be doing so for precisely the reasons that countries give foreign aid: as an act of charity, or solidarity or to bolster its “soft power” on the global stage.
Where, then, should countries draw the line? Which expenditures can be justified as a matter of domestic national priority, as opposed to solidarity or projecting soft power? This is determined by a national investment threshold, which will be different for each country. The total international spend that can be justified as additional to foreign aid1 is articulated by the place on the X-axis at which the national investment threshold crosses the cost curve (i.e. the downward slope of the boxes).
Identifying this national investment threshold and making the case for what should rise above it is crucially important if we want to convince major donor countries to increase international spending. But consider how much more important it is for countries that are not currently donors, or at least not at scale.
For a country like the US, there is around $42 billion annually in foreign aid that can be allocated to the issues that do not make it above the line. For Japan, it’s a little under $18 billion. But these numbers rapidly fall when you move outside the G7 economies that make up just 27% of global GDP (and falling), but provide three-quarters of foreign aid. Middle- and low-income countries already produce a third more GDP than the G7. They may have less spare cash, as they have eight times as many people to look after. But it is not credible that we will tackle global problems if we do not have their sincere engagement, including but not limited to financial contributions.
Yes, we should encourage growing middle-income countries to become donors and give money in foreign aid. But the most effective way of ensuring significant international contributions to solving global challenges like pandemics and climate change from countries like Mexico, Brazil, Malaysia and Indonesia is to identify those expenditures that can be justified as a national priority. In other words, to build their Country Cost Curve for International Spending, and make the case for expenditures that rise above their national investment threshold.
This is not just an exercise in mapping reality (although it will be extremely powerful in that regard). It needs to become an advocacy tool. The question is not only: what is your national investment threshold, and what currently rises above it? It is also: how can we get that threshold down, convincing more countries to cover more of the costs of more international priorities? After all, as the cost curve shows, these expenditures all have a non-zero return to the paying country, in addition to the extraordinary benefits they bring to other specific countries, and the world at large.
We argue that the national investment threshold is determined by four main factors. First, and most obvious is fiscal space. The more money a government has in the kitty, the lower its threshold will be for spending some of that money on international priorities.
Second is the credibility of the return on investment. During the pandemic, neither the return on investment of vaccine R&D nor on getting vaccines out to poorer countries were clear. In a situation of uncertainty, the importance of R&D was so obvious that it still passed the threshold, but vaccinating poor countries did not. In a private meeting, a senior UK government official rejected the self-interest case for the vaccinating poor countries, stating, “whatever you tell me about the economic benefits to this country of vaccinating the world, I won’t believe you.” This official (and doubtless many others) had been led to such a point of cynicism by the scarcely-credible advocacy line of “spend billions to save trillions” that he was no longer in listening mode. If he had been convinced that the benefits to the UK really were 12 times the costs, he might have reached into budgets beyond foreign aid, and funded COVAX properly.
Third is the credibility of the system to deliver. Even if vaccinating the world will save me money, who is to say that stumping up the money will lead to that happening? Again the case of COVAX is salutary. There were many concerns about the willingness of people in low-income countries to take COVID-19 vaccines, as well as their health systems’ ability to get needles into arms. But the biggest barrier to delivery in 2021 ended up being the Indian export ban. We need strong, credible institutions and systems at the global, regional and national level that will give confidence to payers that the potential return on investment will be realized in practice.
Finally, there is worldview. We are dealing here with investments that will benefit other countries at least as much, often much more, than the paying country. It goes without saying that protecting Africans against COVID-19 stood to benefit Africa far more than Europe or North America. How acceptable is that positive externality? Governments with a rivalrous worldview will discount benefits to others from their own return on investment. They will be concerned about other countries unfairly taking advantage of their expenditure, and worried that other countries may pull ahead of them in a zero-sum contest between nations. This will raise their national investment threshold, ensuring that only the highest priorities are funded. On the other hand, governments with a worldview that stresses interdependence and solidarity will see the self-interest case as an added benefit and will tolerate spending where the self-interest case is lower.
If these are the factors that influence the national investment threshold, then the task for advocates is clear. They should focus on countries with growing fiscal space (including outside the G7). They should pour effort into increasing the detail, credibility, and force of the self-interest return-on-investment case for international spending (and stay away from poorly evidenced exaggerations). They should work to remove the barriers that reduce the effectiveness of delivery systems. And they should tirelessly make the case for a worldview based on interdependence and solidarity, not rivalry.
The starting point is to move beyond the binary language of “Global Public Goods” vs “Development Cooperation” and do the hard work of mapping out the Scale of Global Common Benefit, through Country Cost Curves for International Spending.
Return on investment is usually associated with 3-5 year policy and funding cycles. How does one make the case for longer term investments (in say CRVS or, in this case, stronger health systems)? How does one make the case that long-term investing in public health will save money that in future will be ploughed (profitably?) into chasing diseases?